Ascites Treatment & Management: Medical Care, Surgical Care, Diet
Medical Care
Sodium restriction (20-30 mEq/d) and diuretic therapy constitute the standard medical management for ascites and are effective in approximately 95% of patients. Note the following:
Water restriction is used only if persistent hyponatremia is present (see Diet, below).
Patients with ascites and hyponatremia may be treated with aquaretics—vasopressin V2-receptor antagonists that promote excretion of electrolyte-free water. [15] Tolvaptan has been approved by the FDA for treating hypervolemic hyponatremia in ascites. Conivaptan has been approved by the FDA for treating hypervolemic hyponatremia in syndrome of inappropriate antidiuretic hormone; however, studies specific to efficacy in cirrhosis are lacking. [16]
In a multicenter study that assessed the safety and efficacy of an automated pump system for the treatment of refractory ascites in 40 patients at 9 centers, Bellot et al reported the automated pump was an efficacious tool to remove ascites from the peritoneal cavity to the bladder. [17] During the 6-month follow-up period, 90% of the ascites was removed with the pump system; there was also a significant reduction in the monthly median number of large volume paracentesis as well as a reduction in the number of cirrhosis-related adverse events. [17]
Therapeutic paracentesis may be performed in patients who require rapid symptomatic relief for refractory or tense ascites. When small volumes of ascitic fluid are removed, saline alone is an effective plasma expander. [18] The removal of 5 L of fluid or more is considered large-volume paracentesis. [2] Total paracentesis, that is, removal of all ascites (even >20 L), can usually be performed safely.
Supplementing 5 g of albumin per each liter over 5 L of ascitic fluid removed decreases complications of paracentesis, such as electrolyte imbalances and increases in serum creatinine levels secondary to large shifts of intravascular volume. Note: The AASLD indicates that postparacentesis albumin infusion may not be necessary for a single paracentesis of less than 4 to 5 L ((class I, level C recommendation); however, for large-volume paracenteses, an albumin infusion of 6-8 g per liter of fluid removed appears to improve survival and is recommended (class IIa, level C recommendation). [19]
To avoid exposing patients to blood products, the use of terlipressin (eg, 1 mg every 4 hours for 48 hours) rather than albumin has been proposed for prevention of circulatory dysfunction after large-volume paracentesis. Initial studies suggest that terlipressin is as effective as albumin for this purpose. [20, 21]
Repeated therapeutic paracentesis can be used to treat refractory ascites (class I, level C recommendation). [19] For palliative care in patients with advanced cancer, an alternative to serial paracenteses is placement of an indwelling peritoneal catheter; ascitic fluid can then be removed by continuous drainage [22] or intermittent drainage with a proprietary system utilizing vacuum bottles, which can be performed in the patient's home. [23] Preservation of good nutrition status is important. [24]
The transjugular intrahepatic portosystemic shunt (TIPS) is an interventional radiologic technique that reduces portal pressure and may be the most effective treatment for patients with diuretic-resistant ascites. In the procedure, which is performed with the patient under conscious sedation or general anesthesia, an interventional radiologist places a stent percutaneously from the right jugular vein into the hepatic vein, thereby creating a connection between the portal and systemic circulations. TIPS is gradually becoming the standard of care in patients with diuretic-refractory ascites.
In a systematic review and meta-analysis of 10 trials comprising 462 patients with cirrhotic ascites, Guo et al reported that midodrine, a vasopressor, used as a novel therapy for the ascites caused by cirrhosis did not improve survival but potentially improved response rates and reduced plasma renin activity. [25] However, when midodrine was used as an alternative to albumin in large-volume paracentesis, the mortality was higher for those receiving midodrine than for those receiving albumin; midodrine and albumin had a similar association with the development of paracentesis-induced circulatory dysfunction. [25]
Conservative management appears to be the treatment of choice for patients with chylous ascites. [3]
Patients can actually be maintained free of ascites if sodium intake is limited to 10 mmol/d. However, this is not practical outside a metabolic ward.
Twenty-four–hour urinary sodium measurements are useful in patients with ascites related to portal hypertension in order to assess the degree of sodium avidity, monitor the response to diuretics, and assess compliance with diet.
For grade 3 or 4 ascites, therapeutic paracentesis may be necessary intermittently.
Consultation with a gastrointestinal specialist and/or hepatologist should be considered for all patients with ascites, particularly if the ascites is refractory to medical treatment.
Surgical Care
The peritoneovenous shunt is an alternative for patients with medically intractable ascites. This is a megalymphatic shunt that returns the ascitic fluid to the central venous system. Beneficial effects of these shunts include increased cardiac output, renal blood flow, glomerular filtration rate, urinary volume, and sodium excretion and decreased plasma renin activity and plasma aldosterone concentration. Although it has largely been supplanted by transjugular intrahepatic portosystemic shunt (TIPS), peritoneovenous shunting has been shown to improve short-term survival (compared with paracentesis) in cancer patients with refractory malignant ascites. [26] The AASLD suggests considering peritoneovenous shunting for patients with refractory ascites who are not candidates for paracentesis, transplant, or TIPS (class I, level A recommendation). [19]
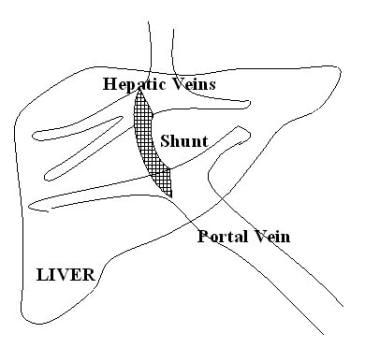
Ascites. Transjugular intrahepatic portosystemic shunt (TIPS).
The AASLD recommends that patients with cirrhosis and ascites be considered for liver transplantation (class I, level B recommendation). [19]
Diet
Sodium restriction of 500 mg/d (22 mmol/d) is feasible in a hospital setting; however, it is unrealistic in most outpatient settings. A more appropriate sodium restriction is 2000 mg/d (88 mmol). Indiscriminate fluid restriction is inappropriate. Fluids need not be restricted unless the serum sodium level drops below 120 mmol/L.
Long-Term Monitoring
The best method of assessing the effectiveness of diuretic therapy is by monitoring body weight and urinary sodium levels.
In general, the goal of diuretic treatment of ascites should be to achieve a weight loss of 300-500 g/d in patients without edema and 800-1000 g/d in patients with edema.
Once ascites has disappeared, diuretic treatment should be adjusted to the minimum effective dose to avoid recurrences. [14]
Chiejina M, Kudaravalli P, Samant H. Ascites. StatPearls [Internet]. 2023 Jan. [QxMD MEDLINE Link]. [Full Text].
Pericleous M, Sarnowski A, Moore A, Fijten R, Zaman M. The clinical management of abdominal ascites, spontaneous bacterial peritonitis and hepatorenal syndrome: a review of current guidelines and recommendations. Eur J Gastroenterol Hepatol. 2016 Mar. 28(3):e10-8. [QxMD MEDLINE Link].
Weniger M, D'Haese JG, Angele MK, Kleespies A, Werner J, Hartwig W. Treatment options for chylous ascites after major abdominal surgery: a systematic review. Am J Surg. 2016 Jan. 211(1):206-13. [QxMD MEDLINE Link].
CDC/National Center for Health Statistics. Chronic liver disease and cirrhosis. Centers for Disease Control and Prevention. January 17, 2023. Available at https://www.cdc.gov/nchs/fastats/liver-disease.htm. Accessed: May 30, 2023.
Raza S, Rajak S, Upadhyay A, Tewari A, Sinha RA. Current treatment paradigms and emerging therapies for NAFLD/NASH. Front Biosci (Landmark Ed). 2021 Jan 1. 26(2):206-37. [QxMD MEDLINE Link]. [Full Text].
Asrani SK, Devarbhavi H, Eaton J, Kamath PS. Burden of liver diseases in the world. J Hepatol. 2019 Jan. 70(1):151-71. [QxMD MEDLINE Link].
Fede G, D'Amico G, Arvaniti V, et al. Renal failure and cirrhosis: a systematic review of mortality and prognosis. J Hepatol. 2012 Apr. 56(4):810-8. [QxMD MEDLINE Link].
Wallerstedt S, Olsson R, Simren M, et al. Abdominal tenderness in ascites patients indicates spontaneous bacterial peritonitis. Eur J Intern Med. 2007 Jan. 18(1):44-7. [QxMD MEDLINE Link].
Tapper EB, Bonder A, Cardenas A. Preventing and treating acute kidney injury among hospitalized patients with cirrhosis and ascites: a narrative review. Am J Med. 2016 May. 129(5):461-7. [QxMD MEDLINE Link].
Han CM, Lee CL, Huang KG, et al. Diagnostic laparoscopy in ascites of unknown origin: Chang Gung Memorial Hospital 20-year experience. Chang Gung Med J. 2008 Jul-Aug. 31(4):378-83. [QxMD MEDLINE Link]. [Full Text].
Wong CL, Holroyd-Leduc J, Thorpe KE, Straus SE. Does this patient have bacterial peritonitis or portal hypertension? How do I perform a paracentesis and analyze the results?. JAMA. 2008 Mar 12. 299(10):1166-78. [QxMD MEDLINE Link].
[Guideline] Biggins SW, Angeli P, Garcia-Tsao G, et al. Diagnosis, evaluation, and management of ascites, spontaneous bacterial peritonitis and hepatorenal syndrome: 2021 practice guidance by the American Association for the Study of Liver Diseases. Hepatology. 2021 Aug. 74(2):1014-48. [QxMD MEDLINE Link]. [Full Text].
[Guideline] Aithal GP, Palaniyappan N, China L, et al. Guidelines on the management of ascites in cirrhosis. Gut. 2021 Jan. 70(1):9-29. [QxMD MEDLINE Link]. [Full Text].
Gallo A, Dedionigi C, Civitelli C, Panzeri A, Corradi C, Squizzato A. Optimal management of cirrhotic ascites: a review for internal medicine physicians. J Transl Int Med. 2020 Dec. 8(4):220-36. [QxMD MEDLINE Link]. [Full Text].
Gines P, Cardenas A. The management of ascites and hyponatremia in cirrhosis. Semin Liver Dis. 2008 Feb. 28(1):43-58. [QxMD MEDLINE Link].
Facciorusso A, Amoruso A, Neve V, Antonino M, Prete VD, Barone M. Role of vaptans in the management of hydroelectrolytic imbalance in liver cirrhosis. World J Hepatol. 2014 Nov 27. 6(11):793-9. [QxMD MEDLINE Link]. [Full Text].
Bellot P, Welker MW, Soriano G, et al. Automated low flow pump system for the treatment of refractory ascites: a multi-center safety and efficacy study. J Hepatol. 2013 May. 58(5):922-7. [QxMD MEDLINE Link].
Sola-Vera J, Minana J, Ricart E, et al. Randomized trial comparing albumin and saline in the prevention of paracentesis-induced circulatory dysfunction in cirrhotic patients with ascites. Hepatology. 2003 May. 37(5):1147-53. [QxMD MEDLINE Link]. [Full Text].
[Guideline] Runyon BA, American Association for the Study of Liver Diseases. Management of adult patients with ascites due to cirrhosis: update 2012. National Guideline Clearinghouse. Available at https://guideline.gov/content.aspx?id=45103&search=ascites. Accessed: Nov 6, 2014.
Lata J, Marecek Z, Fejfar T, et al. The efficacy of terlipressin in comparison with albumin in the prevention of circulatory changes after the paracentesis of tense ascites--a randomized multicentric study. Hepatogastroenterology. 2007 Oct-Nov. 54(79):1930-3. [QxMD MEDLINE Link].
Singh V, Kumar R, Nain CK, Singh B, Sharma AK. Terlipressin versus albumin in paracentesis-induced circulatory dysfunction in cirrhosis: a randomized study. J Gastroenterol Hepatol. 2006 Jan. 21(1 pt 2):303-7. [QxMD MEDLINE Link].
Mercadante S, Intravaia G, Ferrera P, Villari P, David F. Peritoneal catheter for continuous drainage of ascites in advanced cancer patients. Support Care Cancer. 2008 Aug. 16(8):975-8. [QxMD MEDLINE Link].
Courtney A, Nemcek AA Jr, Rosenberg S, et al. Prospective evaluation of the PleurX catheter when used to treat recurrent ascites associated with malignancy. J Vasc Interv Radiol. 2008 Dec. 19(12):1723-31. [QxMD MEDLINE Link].
Sorrentino P, Castaldo G, Tarantino L, et al. Preservation of nutritional-status in patients with refractory ascites due to hepatic cirrhosis who are undergoing repeated paracentesis. J Gastroenterol Hepatol. 2012 Apr. 27(4):813-22. [QxMD MEDLINE Link].
Guo TT, Yang Y, Song Y, Ren Y, Liu ZX, Cheng G. Effects of midodrine in patients with ascites due to cirrhosis: Systematic review and meta-analysis. J Dig Dis. 2016 Jan. 17(1):11-9. [QxMD MEDLINE Link].
Seike M, Maetani I, Sakai Y. Treatment of malignant ascites in patients with advanced cancer: peritoneovenous shunt versus paracentesis. J Gastroenterol Hepatol. 2007 Dec. 22(12):2161-6. [QxMD MEDLINE Link].
Hoorn EJ, Zietse R. Diagnosis and treatment of hyponatremia: compilation of the guidelines. J Am Soc Nephrol. 2017 May. 28(5):1340-1349. [QxMD MEDLINE Link]. [Full Text].
Liu YB, Chen MK. Epidemiology of liver cirrhosis and associated complications: current knowledge and future directions. World J Gastroenterol. 2022 Nov 7. 28(41):5910-30. [QxMD MEDLINE Link]. [Full Text].
Tay PWL, Xiao J, Tan DJH, et al. An epidemiological meta-analysis on the worldwide prevalence, resistance, and outcomes of spontaneous bacterial peritonitis in cirrhosis. Front Med (Lausanne). 2021. 8:693652. [QxMD MEDLINE Link]. [Full Text].
Author
Coauthor(s)
Janice M Fields, MD, FACG, FACP Assistant Professor of Internal Medicine, Oakland University William Beaumont School of Medicine; Consulting Staff, Department of Internal Medicine, Section of Gastroenterology, Providence Hospital, St John Macomb-Oakland Hosptial
Janice M Fields, MD, FACG, FACP is a member of the following medical societies: American College of Gastroenterology, American College of Physicians-American Society of Internal Medicine, American Gastroenterological Association, American Medical Association, American Society for Gastrointestinal Endoscopy, National Medical Association
Disclosure: Nothing to disclose.
Specialty Editor Board
Francisco Talavera, PharmD, PhD Adjunct Assistant Professor, University of Nebraska Medical Center College of Pharmacy; Editor-in-Chief, Medscape Drug Reference
Disclosure: Received salary from Medscape for employment. for: Medscape.
Chief Editor
相关知识
Chronic Disease Management in Omaha, Fremont, Lincoln
Chronic Care Management
Medical Treatment of Pediatric Sinusitis Medication: Antibiotics
Chronic Care Management for Partners
Construction of an Innovative Model of Chronic Disease Management in Compact County Medical Alliance with Treatment
Center for Family Medicine and Integrative Health Care
Implementation and research of social medical treatment health care system middleware based on Web
Medical Care for Addiction
People with Chronic Health Problems Are Heaviest Users of Medical Care, but System Not Organized to Meet Their Needs
医疗保健,Medical care英语短句,例句大全
网址: Ascites Treatment & Management: Medical Care, Surgical Care, Diet https://m.trfsz.com/newsview1300532.html